






 Information in English
Information in English















The problem of unsafe abortion
Momade Bay Ustá
There is an old African saying “Every pregnant woman has one foot in the grave”. This was true in our grandparents’ time but unfortunately it is still true today. This article tries to consider the constant presence of unsafe abortion, while at the same time discussing its frequency, consequences and the alternatives for eradicating it.
Unsafe abortion continues to be a reality in the 21st century
Given the growing number of deaths from unsafe abortion and the enormous maternal mortality rate, we must ask ourselves: must it be so in the 21st century, when there is scientific knowledge and technology to provide full quality reproductive health services, including safe abortion? How and how early must we work to improve the situation?
While we wait and do not take the necessary measures, every year thousands and thousands on our continent die because they do not have access to safe abortion services. This situation is related to various factors.
Firstly, they do not have access to effective contraceptives. To have an idea, the average prevalence of contraceptives in Africa is less than 15%[1]; in Mozambique the total Contraception Prevalence rate rose to 17% in 2003 – 29% in urban areas and 12% in rural areas.
A second factor related to lack of access to services providing safe abortion is the stigma and silence that surrounds it, not only among the population in general but also among health professionals.
A third factor relates to gender inequalities because, despite major social changes throughout the continent, women do not have a say in their Reproductive Health.
A fourth factor is ignorance among policymakers, legislators, health professionals and unfortunately women themselves. By this we mean myths and beliefs that associate abortion with depravity, customs or other evils, reinforced by hypocrisy, fundamentalism, religion and dogma.
Until a short time ago, the fifth factor was USA policy that penalised programmes fighting for the decriminalisation of abortion by withdrawing funding from them. The USA thus denied African women the rights that American women have.
Finally, and no less important, there were primitive, archaic colonial laws dating back to the 19th century, as in the case of Mozambique, or other legislation criminalising abortion.
We must all understand what is meant by unsafe abortion. WHO (2003) has defined it as follows:
The interruption of pregnancy carried out by persons lacking the necessary skills or in an environment that does not conform to medical and hygiene standards or both.
According to WHO data (2011) every year 46 million pregnancies are terminated through induced abortion. It is estimated that roughly half of these abortions, corresponding to 1/10 of all pregnancies, are unsafe. WHO also estimates that:
- 4.2 million African women have an unsafe abortion every year;
- Many are brought about by the women themselves. Some of the most common methods used either by women or buy abortionists include: inserting into the uterus catheters, sticks or roots, crochet hooks and other types of objects; ingesting drinks made of herbs that are often poisonous; caustic substances such as bleach or even chloroquine (Walker, 2008).
Many of these methods do not have the desired effect and are often associated with a woman’s death.
Abortions take place throughout the world irrespective of the legal situation or other factors. The tragedy is that almost all unsafe abortions take place in developing countries (and “transitional” countries as in Eastern Europe and the former Soviet republics). There are, of course, virtually no unsafe abortions in developed countries where safe abortion is usually available legally (WHO, 2003). There is no “typical” group of women who have abortions; they occur in all age groups, across a wide variety of women and Mozambique is no exception.
Based on studies in 56 countries, the highest proportion of abortions take place among women aged 20-24 and 25-29 (Bankhole et al., 1999). To a large extent this model reflects the lower fertility among younger and older women. When women in the younger and older age groups become pregnant, they probably resort to an abortion more frequently than middle-aged women.
The overall impact of unsafe abortion is serious. It is calculated that:
- There are 200 deaths a day throughout the world due to unsafe abortions;
- 99.9% of complications and deaths occur in the developing world; about 44% of the global maternal mortality due to abortion is in Africa – roughly 90 African women die every day;
- These percentages can be higher in some regions and countries; in some African countries the figure reaches 50% (WHO, 1998).
All these deaths are unnecessary. Safe abortion is one of the safest medical procedures in the world.
Why do women decide to have an abortion? What are the consequences of an unsafe abortion?
A wide range of women seek abortions. Their profile tends to vary from region to region and depends on a variety of factors, including average age at marriage, prevalence of sexual activity before marriage, access to contraception, expectations about the ideal family size, among others. There are many reasons why a married woman decides to interrupt her pregnancy (Bankhole et al., 1999).
Women may not want to be pregnant for a variety of reasons (WHO, 2003), namely:
- Personal reasons
- Health reasons
- Socioeconmic reasons
- Cultural reasons
- Being in an unstable relationship
- Not wanting to have more children or spacing
- The pregnancy might not be supported by the partner, family or community.
In addition to death, the consequences of an unsafe abortion can be very serious. An unsafe abortion can lead to:
- Serious short-term and long-term illness and lesions for the woman;
- Infertility, a very serious problem in Africa;
- High hospital costs to treat complications;
- Negative impacts on the women, families, children and the community;
- Higher probability of death among children whose mothers die.
The most common complications include perforation of the uterus, haemorrhage, and infections of various types and severity.
Unsafe abortion also has a very serious economic impact on the health system, requiring substantial budget expenditure that could have been spent on important health programmes such as reproductive and neonatal health programmes and even HIV/AIDS.
There is an enormous negative impact on families given the high probability of malnutrition, interruption of education opportunities and their mothers’ reduced ability to contribute to her family’s well-being for children whose mothers die while trying to have an abortion.
A country’s legal restrictions on abortion do not necessarily reduce their number. It merely means that they are concealed and unsafe and the women who resort to these services pay a heavy price, including risking their lives! Where abortion is legal there are safe services, and a substantial reduction in deaths and incapacity due to abortion. Although the liberalisation of abortion does not necessarily mean that women can gain access to safe abortion, there is frequently a correlation between the two. The following table shows the example of Romania:
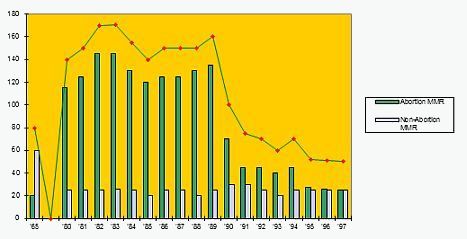
During the time of the dictator Ceausescu, between 1966 and 1989, there were very strong restrictions on abortion. After he was deposed, abortion was legalised in December 1989 and in early 1990 there was a drastic reduction in maternal mortality, with deaths due to unsafe abortion the main reason. The table shows this decline since 1989 (Scarlat, 2005).
Over the last two decades, 17 countries in the world have revised their laws to make them less restrictive. When this is accompanied by an expansion of safe services, as happened in South Africa, legalisation on abortion reduces considerably the resulting complications and deaths. In South Africa, following a change in the law in 1997 abortion related deaths fell by 91% (Jewkes et al., 2005).
But unsafe abortion is not just a health problem. It is also a social injustice problem that requires action by governments, policy makers, donors and communities. An unwanted pregnancy and unsafe abortion are both a violation of women’s basic human rights. Women and married couples have the right to decide when they want to have children and the size of their families.
It is also a social injustice problem because it affects proportionately the poorest and thus the most vulnerable. Throughout the world, even in countries where laws are very restrictive, women in a good economic situation can obtain a safe abortion. Poor women, adolescents, refugees and other kinds of vulnerable populations rarely have this option. These are the women who often resort to an unsafe abortion for the good of their future, their families and their children. Unfortunately, they are also the ones who pay the highest price – health problems and even death.
Finally, it must be emphasised that unsafe abortion is not “just a woman’s problem”, as it has very serious effects for their families and for communities.
Independent studies (Machungo et al., 1997) analysing maternal mortality in Maputo Central Hospital (HCM) between 1990 and 1999 have shown the following:
- 540 maternal deaths (11%) were related to an unsafe abortion (but this percentage could be just the tip of the iceberg). Many happen at home and are not recorded as such. The average age was 23 years; 63% of the women who resorted to an unsafe abortion had little education; 75% were single; 29% were from suburban neighbourhoods; 88% were from low income families;
- 1 in 30 women who had an unsafe abortion died;
- No women who had an abortion in the hospital died;
- Most women who resorted to unsafe abortions knew less about contraceptives and used them less.
What are the alternatives for eradicating unsafe abortion?
Virtually all countries SHOULD offer safe abortion services. National legislation also varies a great deal, although almost all countries in the world provide some space for abortion under very specific circumstances:
- To save the lives of mothers – almost all;
- To preserve physical and mental health – 60% of countries;
- In cases of rape, incest and foetal anomalies – about 40%.
Nevertheless, despite this, many women cannot exercise their right to safe abortion for a variety of reasons, including:
- Lack of information – providers, women and communities do not know the law; no dissemination;
- Cost – usually high (for example, the cost can include transport to the health unit, expenditure on consultations and accommodation);
- Social attitudes – religion, stigma and culture;
- Health system – lack of trained personnel, equipment and resources;
- Political issues – administrative, judicial and regulatory barriers.
A multi-sector working group legitimised by the Council of Ministers was formed in 2005 with the following objectives:
- To study under which conditions abortion should be decriminalised;
- To produce a bill within the overall context of the country’s on-going law reform;
- To lead an open and inclusive debate to gather political, religious and civil society’s feelings.
Following debate throughout the country the group produced a document that reflected its consensus on a future law on abortion:
- Most people were in favour of total freedom for abortion in selected units;
- Permission for abortion would cover the following situations: saving the mother’s life, incest, rape, economic reasons.
Policymakers should clarify the legal aspects of the supply of safe abortion to remove administrative barriers and regulations.
The Millennium Development Goals (MDG) were developed following adoption of the Millennium Declaration by 189 world leaders meeting in a Special United Nations General Assembly in September 2000. Based on various international conferences held in 1990, they oblige member states and the international community to fight poverty and promote human development.
The fifth and eighth targets appeal to world governments to reduce the maternal mortality rate by three quarters between 1990 and 2015.
Of the various direct and indirect causes of maternal deaths – that include obstructed birth, sepsis, haemorrhage and conditions such as malaria that can be worse during pregnancy – unsafe abortion is probably the cause that is technically the easiest to correct in some places. In some countries, it is estimated that unsafe abortion can account for half of maternal deaths. In these cases, the MDGs cannot be achieved unless the problem of unsafe abortion is addressed (UN, 2000).
“Women are not dying from diseases that cannot be treated. They are dying because society still has to take the decision that their lives are worth saving”.
Dr. Mahmoud Fathalla
References:
- Bankole, A.; S. Singh; T. Haas (1999), “Characteristics of Women Who Obtain Induced Abortion: A Worldwide Review”. In: International Family Planning Perspectives, 25 (https://www.guttmacher.org/pubs/journals/2506899.html)
- Jewkes, R.; Rees, H.; Dickson, K.; Brown, H.; Levin, J. (2005). “The impact of age on the epidemiology of incomplete abortions in South Africa after legislative change”. In: BJOG 112 (3). pp. 355–9
- Machungo, F.; Zanconato, G.; Bergstrom, S. (1997), Reproductive characteristics and post-abortion health consequences in women undergoing illegal and legal abortion in Maputo. In: Soc Sci Med, 45 (11). pp. 1607-13
- Scarlat, S. (2005), “‘Decretei’: produsele unei epoci care a îmbolnavit România” (“‘Scions of the Decree’: Products of an Era that Sickened Romania”). In: Evenimentul Zilei, May 17
- UNO (2000), United Nations Millennium Declaration, Millennium Assembly of the United Nations, Sept. 6-8, 2000 (New York: United Nations, 2000).
- Walker, Andrew (2008), “Saving Nigerians from risky abortions“. BBC News, acedido a 31/05/2009
- WHO (1998). Unsafe abortion. Global and regional estimates of incidence of and mortality due to unsafe abortion with a listing of available country data. Third edition. Geneva: World Health.
- WHO (2003), Safe Abortion: Technical and Policy Guidance for Health Systems. In: http://www.who.int/reproductivehealth/publications/unsafe_abortion/9789241548434/en/. (2nd ed.; 2012)
- WHO (2011). “Preventing unsafe abortion” (World Health Organization 2011): In: http://www.who.int/reproductivehealth/publications/unsafe_abortion/en/, accessed April 7, 2013.
- Population Reference Bureau (PRB) (2002), Family planning worldwide. Washington, DC.
* * *